 Overview
OverviewOctober 1, 2024

Prof. Prof. DK Prof. Dr. med. Marc Possover, MD, PhD
25 Years of Experience - Why Outcomes Depend on Neuropelveological Mastery
The Possover Weekly Neuropelveological Reference
Prof. Marc Possover
Endometriosis of the sciatic nerve is universally considered a rare disease. In classical gynecology, it is still often regarded as anecdotal.
Yet over the last 25 years, more than 500 women have undergone laparoscopic surgery for sciatic nerve endometriosis in our center alone.
This number is not the reflection of a rising prevalence - it is the reflection of historical exclusivity.
I began performing laparoscopic surgery of the pelvic nerves in 2004, at a time when endometriosis of the sciatic nerve was considered almost impossible. Many colleagues predicted that my patients would “leave in a wheelchair.”
The opposite happened.
Today, the concept of sciatic nerve endometriosis surgery has become fashionable.
But in parallel, I now see a growing number of recurrences and failed re-operations performed elsewhere - something that has never occurred in my own patients.
This contradiction reveals a fundamental truth: Sciatic nerve endometriosis is not a gynecologic disease. It is a neuropelveological disease requiring microsurgical nerve and vascular mastery.
In the largest long-term series ever published on this pathology with more than 500 cases, including 259 consecutive patients operated between 2004 and 2016, we analyzed neurological and functional outcomes after laparoscopic sciatic nerve surgery.
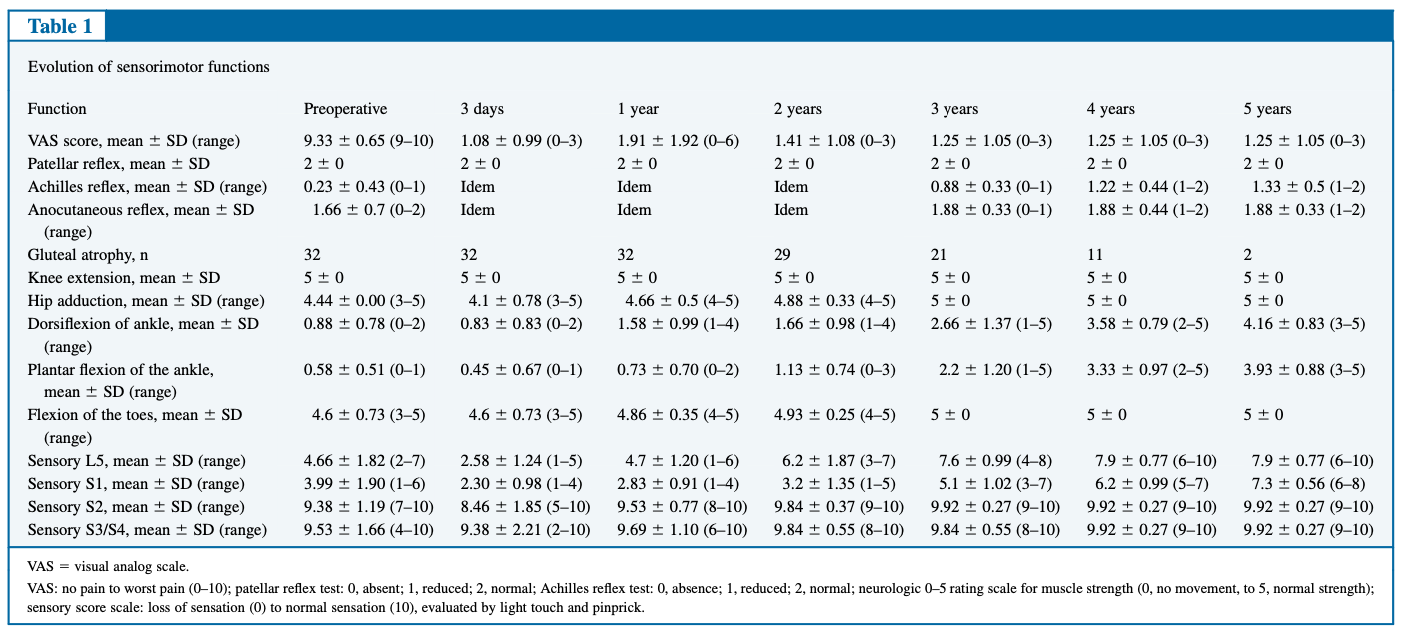
In the subgroup requiring large intraneural nerve resections (>30% of the nerve), all patients presented preoperatively with:
Despite this, five-year follow-up demonstrated:
These outcomes are unique in nerve surgery and impossible to reproduce without deep neuropelveological expertise.
Sciatic nerve endometriosis is not superficial pelvic endometriosis.
It is intraneural, perineural and vascular.
The main danger is not the nerve itself, it is the pelvic vessels entangling the nerve and the massive retroperitoneal fibrosis surrounding it.
I was trained as a cardiovascular surgeon before becoming a gynecologic surgeon.
This vascular mastery became the cornerstone of my neuropelveological approach.
Most surgeons performing “modern sciatic endometriosis surgery” are not trained to:
Incomplete surgery = persistent disease = recurrence.
Sciatic nerve endometriosis can involve:
The surgical access route changes completely depending on the topographic level of involvement. Without a neuropelveologic work-up, the surgeon operates blindly.
This is why classical MRI and gynecologic diagnostics frequently fail, and why patients wander for years before diagnosis.
This surgery is not gynecology. It is microsurgical nerve and vascular surgery in the pelvis and requires
These elements cannot be replaced by robotics. Laparoscopy remains the only approach that allows safe, tactile, neurovascular microsurgery inside the pelvis.
Sciatic nerve endometriosis surgery is not a trend.
It is a discipline. And disciplines require founders, not followers.
For 25 years, neuropelveology has defined the standards that now, belatedly, the world is beginning to discover. What appears “new” today is simply what was built two decades ago.
And what appears “rare” is simply what only one center has truly mastered over the last 20 years.
— Prof. Marc Possover
Founder of Neuropelveology
We’re Here to Help
Possover International Medical Center – Zurich
☎️ +41 44 520 3600
📍 Klausstrasse 4, CH-8002 Zürich
🌐 www.possover.com
📧 mail@possover.com
Let us help you find the cause of your pain - and finally start your journey toward healing.
If you or someone you know is struggling with chronic pelvic pain, pelvic nerve disorders, endometriosis, or consequences of pelvic surgery, please contact us via email at international@possover.com to begin the process. Because we want to avoid the scenario where a patient travels to Zurich, only to discover that we may not be able to offer help for their specific situation, we have Pre-Consultation Zoom process. How does it work?